Lumbar spinal stenosis (LSS) is a condition in which the spinal canal becomes increasing narrowed from degenerative changes. Patients with LSS may experience symptoms of neurogenic claudication, including pain or discomfort that radiates to their lower leg, thigh, and/or buttocks while walking. Patients with more pronounced LSS report symptoms of develop lower extremity of weakness, muscle cramping, numbness, and imbalance. LSS is a debilitating, degenerative condition that worsens over time when left untreated.1 Because of the dynamic nature of LSS, the pain is worsened when walking or standing, and relieved when bending forward, sitting or in the forward flexing position.
Offering an alternative option for the symptomatic LSS patient, which restores functional capacity and alleviates back and leg pain as well as other associated symptoms such as cramping, numbness and weakness without the reliance on medication is a much-needed therapy option.
The Ohio Society of Interventional Pain Physicians supports the use of the SuperionTM Indirect Decompression Systems (IDS) as an option for the treatment of lumbar stenosis patients as it augments the prevailing solutions and reaches additional patients who would otherwise be left untreated.
Interspinous spacer decompression using the Superion device offers a less invasive procedure for patients who fail conservative treatment before traditional more invasive surgery. It serves as an extension blocker, which in turn relieves pressure on the affected nerves, helping to minimize the clinical impact of dynamic spinal stenosis while fully preserving the patient’s nascent architecture and anatomy.2 Superion’s mechanism of action addresses the root cause of stenosis in moderately stenosed patients rather simply palliating the symptoms. Its effectiveness mirrors those of the most invasive procedures, without exposing patients to longer recovery times, complication risks. It provides an option to those too frail to undergo more invasive procedures because it preserves the spinal anatomy for the patient as well as the surgeon should a future decompression become necessary.
PROCEDURE
The Superion ISS may be implanted at one or two adjacent lumbar levels in patients whom treatment is indicated and at no more than two levels, from L1 to L5. The device is inserted through a cannula about the size of a dime and thus requires no surgical dissection of the spinal musculature. The procedure is performed in an outpatient setting or ASC. The device may be implanted by an interventional pain specialist or a surgeon.
FDA INDICATION AND LABELING
The Superion ISS received FDA approval in 2015 based on a prospective, multi-site randomized clinical trial of Superion (n=190 patients) versus XSTOP (n=201 patients) with 3 year follow up.3
“This device is indicated to treat skeletally mature patients suffering from pain, numbness, and/or cramping in the legs (neurogenic intermittent claudication) secondary to a diagnosis of moderate degenerative lumbar spinal stenosis….
Impaired physical function who experience relief in flexion from symptoms of leg/buttock/groin pain
numbness and/or cramping with or without back pain
patients have undergone at least 6 months of non-operative treatment
CLINICAL EVIDENCE
The Vertiflex procedure is supported by 5 Year Level 1 Evidence. At 3 years, Superion (63/120, 52.5%) vs X STOP (49/129, 38%), (P=.023) achieved the desired endpoint and maintained improvement in back and leg pain.
Success rate > 80% for each component of the primary endpoint in the Superion Group. (Range: 81%-91%).
NOTE: Primary composite endpoint: Improvement in two of three domains of the Zurich Claudication Questionnaire, no reoperations at the index level, no major implant-or procedure related complications, and no clinically significant confounding treatments.
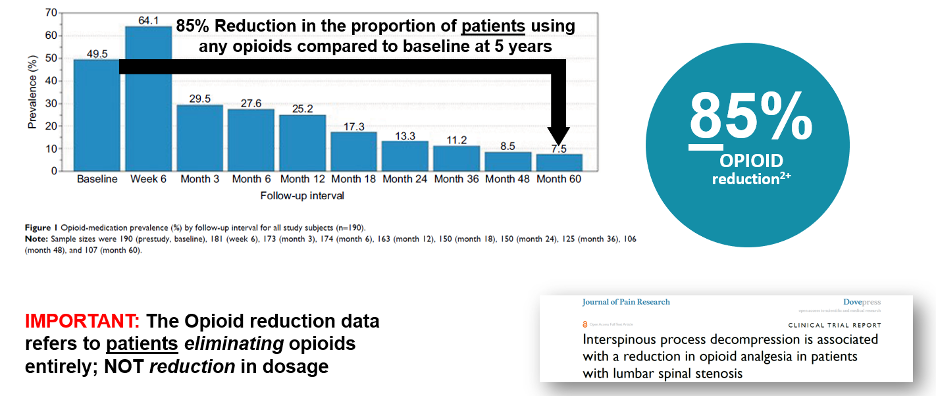
Nunley (2018) reported on the pattern of opioid use in this pivotal study. At baseline, Nunley (2018) reported 50% (94 of 190) patients were using opioid medication. The study showed a sharp decrease in opioid utilization from 25.2% (41 of 163) at 12 months to 13.3% (20 of 150) at 24 months to 7.5% (8 of 107) at 60 months. 85% reduction in the proportion of patients using opioids compared to baseline at 5 years. 4
Three, four and five year follow up studies of Superion patients demonstrate solid outcomes.
At 5 years post-procedure, there were statistically significant improvements in clinical outcomes (symptom severity and physical function) and severity leg and back pain according to data from a randomized, controlled FDA noninferiority trial. 5

Parker et al. investigated the cost effectiveness of conservative care, laminectomy, and Superion. Although conservative care has the lowest costs ($10,540 USD) it was less effective. On average, the surgeries costs $3400 more per patient than the conservative strategy, with greater QALYs gained of 0.21 to 0.22 6
Early results from an ongoing real-world registry following commercial patients who underwent the Vertiflex Procedure (n=1,523 at 6 mos., 423 at 12 mos.) show 75% of patients enjoying a clinically meaningful reduction in leg pain, 74% report significant functional improvement, an 80% patient satisfaction rate at 12 months post-procedure, and a low (5%) reoperation rate. 7
>> Click here for a printable document.
SOURCES:
Nunley PD, Patel VV, Orndorff DG, et al. Five-year durability of stand-alone interspinous process decompression for lumbar spinal stenosis. Clin Interv Aging. 2017; 12: 1409 – 1417. Doi: 10.2147/cia.s143503.
Vertiflex Superion Interspinous Spacer: PMA No. P140004. https://www.vertiflex.com/wp-content/uploads/2016/09/Superion-PMA-Summary.pdf. Accessed February 26, 2021
FDA P140004 SSED
Nunley PD, Patel VV, Orndorff DG, et al. Interspinous process decompression improves quality of life in patients with lumbar spinal stenosis. Minim Invasive Surg. 2018; 2018: 1035954. Doi: 10.1155/2018/1035954.
Nunley PD, Patel VV, Orndorff DG, et al. Five-year durability of stand-alone interspinous process decompression for lumbar spinal stenosis. Clin Interv Aging. 2017; 12: 1409 – 1417. Doi: 10.2147/cia.s143503.
Parker SL, Anderson LH, Nelson T, Patel VV. Cost-effectiveness of three treatment strategies for lumbar spinal stenosis: conservative care, laminectomy, and the Superion interspinous spacer. Int J Spine Surg. 2015; 9. Doi: 10.14444/2028.
Deer T, et al. The MIST Guidelines: The Lumbar Spinal Stenosis Consensus Group guidelines for minimally invasive spine treatment. Pain Pract. 2018; doi: 10.1111/papr.12744